투구 동작은 6단계
6 phases of throwing

1. Wind-up (와인드 업)
2. Early cocking (초기 코킹 단계)
3. Late cocking (후기 코킹 단계)
4. Acceleration (가속기)
5. Deceleration (감속기)
6. Follow through (팔로우 스루)
이 6단계 동작은 약 2초 동안 빠르게 이루어지며, 특히 이 중 와인드업(wind-up) 과 가속기(acceleration) 단계가 전체의 약 75%(1.5초)를 차지
에너지의 흐름이 하체에서 상체로 올라가서 손끝의 공까지 전달된 후 다시 하체로 내려가는 에너지 흐름(kinematic chain)을 형성하고 있기 때문에 하지와 몸통 전반적인 근육의 기능도 중요
또 동작이 이루어질 동안 견갑골(scapula)과 상완골(humerus)의 운동이 조화를 이루어야 견관절 손상을 예방

1. 와인드업 단계(Wind-up phase)
투구하는 손의 반대편 하지를 들어 올려 잠재적으로 에너지를 누적하는 단계
- 견관절에 걸리는 부하는 미미
- 회전근개가 활성화되기 전단계

2. 초기 코킹 단계(Early cocking phase
운동에너지를 만드는 과정
상지가 외전(abduction), 외회전(ER)
최대 활성화 근육 : 삼각근(deltoid)

3. 후기 코킹 단계 (Late cocking phase)
견관절의 외회전(ER)이 최대
비유 하자면 최대로 태엽이 김겨있는 상태
따라서 매우 높은 토크(Torque)에 의해 견관절에 부하가 가장 크게 걸리는 단계
또한 가속에 의한 peel-back mechanism*으로 인한 부상, 즉 슬랩병변(SLAP lesion)이 가장 많이 발생하는 단계
이 단계에서 크게 부하가 걸리는 구조물들을 살펴보면,
1) 최대 활성화 근육(muscle)
: 극상근(supraspinatus), 극하근(infraspinatus), 소원근(teres minor)
상완골두(humeral head)를 관절와(glenoid)에 안정화 시키기 위해 회전근개 근육이 최대로 활성화(Peak rotator cuff activity)
2) 최대 장력이 걸리는 인대(ligament)
: 견관절의 하방 관절와-상완인대(IGHL; inferior glenohumeral ligament), 주관절의 내측측부인대(MCL; medial collateral ligament)의 전방 밴드(anterior band)에 가장 큰 부하

4. 가속기(Acceleration phase)
손끝으로 회전력이 집중되며 공을 릴리즈(release) 하는 단계
회전속도(혹은 각속도, angular velocity)가 최대이면서 동시에,
1) 견관절이 외회전(ER; external rotation)에서 내회전(IR; internal rotation)로 바뀌는 시기이고
2) 주관절이 신전 (90°~120° 굴곡 상태에서 25°~30°로) 되는 시기
이 단계에서 크게 부하가 걸리는 구조물들을 살펴보면,
1) 최대 활성화 근육(muscle)
초기 : triceps(삼두근) - elbow가 신전(extension)
후기 : pectoralis major(대흉근), latissimus dorsi(광배근), serratus anterior(전거근) - shoulder의 primary internal rotator로 작용
2) 최대 장력이 걸리는 인대(ligament)
이 시기에서 중요한 점은 최고 5000°/s~ 50000°/s의 각속도로 회전을 하면서
동시에 주관절(elbow)이 25°까지 신전(extension) 된다는 점
이때 주관절(elbow)은 외반력(valgus force)을 받게 되면서
내측(medial side) - 내측측부인대(MCL)의 ant. bundle에 신장력(tensile force)이 발생하고
가측(lateral side) - 축성 압박력(axial compressive force)을 받게 된다. 이런 과정들이 반복되면서 여러가지 주관절의 손상이 유발되기 쉽다.

5. 감속기 (Deceleration phase)
무게 중심이 앞발로 옮겨지는 시기
상지운동을 늦추기 위해 모든 근육의 원심성 수축(eccentric contraction)*이 발생
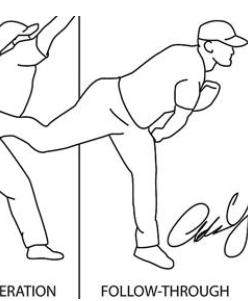
6. 팔로우 스루(Follow through)
공이 나간 후 에너지가 다시 하지로 분산되고 몸통은 재균형을 찾는다.
몸이 더 이상 전방으로 진행하지 않고 멈추며 근육의 활성화도가 정상 레벨
용어정리
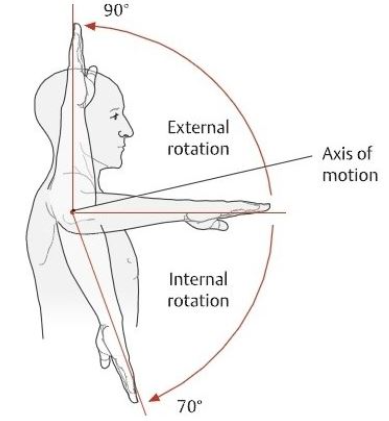
ER : external rotation, 외회전
IR : internal rotation, 내회전
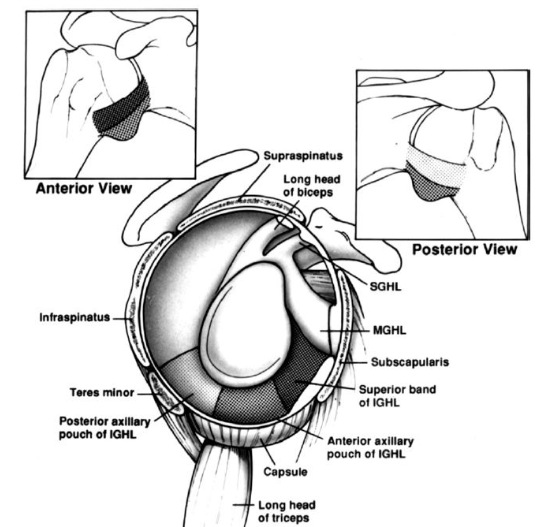
IGHL : inferior gleno-humeral ligament
하방 관절와-상완 인대
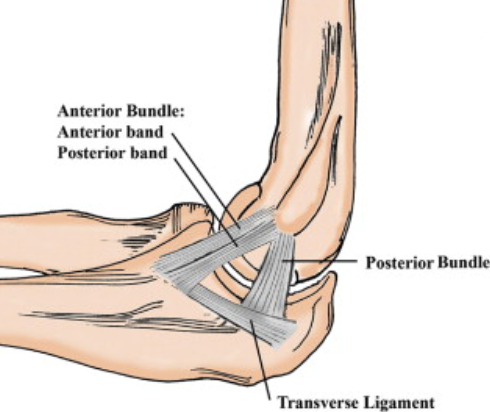
MCL : medial collateral ligament, 내측 측부인대
Introduction

Throwing, for example, baseball pitching, is one of the most intensely studied athletic motions[1]. Although the focus has been more on the shoulder, the entire body movement is required to perform the act of throwing. Throwing is also considered one of the fastest human motions performed, and maximum humeral internal rotation velocity reaches about 7000 to 7500°/second[2].
Phases
The phases of an overhead throw consist of a:
wind-up,
stride,
cocking,
acceleration,
deceleration and
follow through phase [1][3].
Each phase will illustrate the definition, injury occurrence rate, and lastly pathological possibilities.
Wind-Up Phase
The wind-up phase is defined as the initial movement to maximum knee lift of stride leg [3]. During the initial movements, the pitcher brings his or her hands overhead and lowers to chest level. During these simple movements consider the muscles proximally to distally. EMG studies show that the upper trapezius has a maximum voluntary isometric contraction (MVIC) of 18%, serratus anterior 20%, and anterior deltoid 15%. During this phase, the muscle activity is quite low and for these reasons risk of injury is low as well [3].
The pitcher is facing the batter with the baseball concealed away from the batter and in the glove, and both the feet are in contact with the ground. This is known as the wind-up stance[1].
For a right-handed pitcher, throwing arm is the right arm, a gloved hand is left, lead/stride leg is left lower extremity and pivot/stance leg is right.
The phase of wind-up begins with the initiation of the stride leg and ends when the ball separates from the glove and the stride leg reaches the highest point[2].
The ipsilateral leg and trunk rotate approximately 90° and the contralateral hip and knee flex[5].
During the wind-up phase, the energy is transferred from stride leg to pivot leg and winding up of the stride leg occurs. It is an important phase which is responsible for imparting the velocity which is driven to the point of ball release. It is reported that about 50% of the velocity of the ball during an overhead throw is generated from step and body rotation[6]. The body’s overall centre of gravity is raised and minimal stress is imparted on the shoulder during this phase[7].
The purpose of wind-up is threefold:
to establish a rhythm to achieve correct timing for subsequent movements,
to conceal the ball and distract the hitter and
to place the body in a position that may contribute to the propulsion of the ball[5].
Muscle activation
During this phase, there is minimal muscle activity and muscle fire at low intensity[8][9].
As the stride leg is flexed, the weight is transferred from stride leg to pivot leg and hip abductor, adductor and extensors of pivot leg act as weight absorber[1].
Anterior deltoid and pectoralis major work concentrically at the glenohumeral joint. Upper trapezius, serratus anterior and lower trapezius work to produce upward rotation of the scapula. The abdominal muscles work to rotate and stabilize the trunk.
Stride Phase
The picture below depicts an overhead view of the alignment of the body during the acceleration phase of throwing. Note the 15-degree angle of the foot away from the centre of the mound [10]. The stride ankle also typically lands approximately 10cm away from the same midline with a distance from the rubber averaging 87% of the pitcher's height [10]. Fleisig[10] emphasizes the importance of these values by describing the change in force exhibited on the shoulder when they deviate from the norm. During the cocking phase, Fleisig[10] reports a 3.0N increase in anterior force at the shoulder for every extra cm and a 2.1N increase in anterior force at the shoulder with every degree increase of foot angle. Please note that decreasing the distance away from the centre or decreasing the angle did not result in an increased anterior force on the shoulder. So, because of the increased anterior force on the shoulder, it can be assumed that over time the anterior ligamentous structures to the glenohumeral joint may be compromised. This finding is consistent with the anterior glenohumeral instability found in many throwing athletes and emphasizes the importance of proper mechanics throughout the entire kinematic chain [11].
Arm Cocking Phase
Baseball pitch.jpg
The arm cocking phase can be defined as the beginning of lead foot contact and ends at maximum shoulder external rotation [3]. A substantial amount of kinetic energy is transmitted to the shoulder, approximately 80% of body weight, from the lower extremities and trunk rotation. Due to the circumstances, the scapula and shoulder muscles are highly activated to promote and sustain movements of the shoulder, especially external rotation. Special focus on anterior instability in this phase is vital due to the high ranges of external rotation reached in this phase [12] [11]. In a study of pitchers with chronic anterior instability, stimulation of mechanoreceptors within the glenohumeral joint excited and/or inhibited certain muscles. The Biceps Brachii and supraspinatus are shown to be initiated or excited by these mechanoreceptors and assist with the prevention of anterior instability. Over time the excessive utilization of the biceps brachii could lead to a superior labrum anterior to posterior (SLAP) tear. Simultaneously the pectoralis major, subscapularis, and serratus anterior are inhibited. These muscles decelerate shoulder external rotation in this phase. When these actions cannot be performed there is an increased likelihood of anterior instability of the glenohumeral joint [3].
Cocking phase is further divided into (a) early cocking and (b) late cocking.
Early cocking phase
It begins with the end of the windup phase or when the stride leg reaches its maximum height and it ends when the stride leg contacts the mound/ground[1][2].
During an ideal pitch, at this point, the throwing arm is in ‘semi-cocked’ position. With the arm approximately 90° abduction, 30° horizontal abduction, and 50° external rotation[9].
As the ball is removed from the glove, the centre of gravity is lowered by flexing the knee of the pivot leg and the stride leg gradually extends and moves towards the batter[9].
Its main function is to allow a linear and angular motion of the trunk, which lands directly in front of the pivot leg with the toes pointing slightly in[13]. The knee and hip of the pivot leg extend and initiate pelvic rotation and forward tilting followed by upper torso rotation[2].
Muscle activation in Early cocking:
Hip extensors and abductors, knee flexors and ankle plantar flexors of the pivot leg work to propel the weight forward as the stride leg is moving forward. And hip extensors and abductors, knee extensors and ankle plantar flexors of stride leg work eccentrically to control the lowering of body’s centre of gravity. Abdominal obliques work eccentrically to control excess lumbar hyperextension.
In the early cocking phase, the supraspinatus and deltoid work together to abduct the arm with a peak activity [9][14]. And later during the late cocking phase the activity of deltoid decreases.
The other muscles which produce peak activity during early cocking phase are right extensor carpi radialis longus and brevis, extensor digitorum communis, right gluteus maximus and left oblique for right-handed pitcher[1]. And the muscle which produces a strong contraction is left erector spinae and left gluteus maximus for a right-handed pitcher. Whereas trapezius, serratus anterior and pectoralis are moderately active to position the scapula.
Late Cocking phase
This phase begins from the point where the stride leg contacts the ground to the point of maximum external rotation of the throwing arm.
During this phase, the trunk is perpendicular to the batter and upper extremity position is finalized[1]. The pelvis reaches its maximum rotation and the upper torso continues to rotate and tilt forward and laterally.
The shoulder is abducted about 90°, 10° to 20° horizontally adducted and laterally rotates to about 175°. The wrist is in neutral and the elbow is elevated to about shoulder height and is 90° flexed.
During this phase, a varus torque of about 64 N-m is generated at the elbow and about 67 N-m internal rotation torque is generated at the shoulder[15]. The scapula is elevated and upwardly rotated which provides adequate subacromial space to avoid impingement.
Muscle activation in Late cocking:
During the late cocking phase, the pivot leg hip extensor, knee flexor and calf muscles work concentrically to transfer the force up the kinetic chain and aide in force generation at the arm.
Serratus anterior and pectoralis major produce their greatest activity during the late cocking phase just before maximum external rotation[8].
Infraspinatus and teres minor have their peak activity to externally rotate the arm concentrically and later on their activity is decreased to moderate levels during the acceleration phase.
Subscapularis produces significant eccentric contraction as the humerus passes neutral rotation to control the lateral rotation of the arm.
Biceps brachii presents with peak activity during flexion of the elbow in the late cocking phase as it limits anterior translation and compression forces of the humeral head. As the wrist extension reaches a maximum, the wrist extensor is at its greatest activity[5].
Arm Acceleration Phase
The arm acceleration phase begins at maximum shoulder external rotation and ends at ball release [3]. During this phase, it is vital to maintain scapular stabilization due to the forward acceleration of the arm which is equivalent of a peak internal rotation angular velocity of approximately 6500⁰/sec near ball release. Improper stabilization of the scapula may be the cause of the increased risk of shoulder impingement in this phase. Coupled with the arm cocking phase this phase has also been hypothesized to be at increased risk of various shoulder injuries due to the high kinetic energy generated from the lower extremities [3] [11].
The acceleration phase begins from the point of maximum shoulder external rotation to the point of ball release.
The trunk continues to rotate and tilt, and energy transferred through upper extremity.
During this phase, the shoulder moves into horizontal adduction and internal rotation. A rapid shoulder internal rotation takes place and shoulder moves from point of 175o of humeral external rotation to 100o of humeral internal rotation in about 42 to 58 milliseconds[5].
Ball release takes place between 40o and 60o of humeral external rotation. The elbow first moves to about 120o of flexion and then rapidly extends to about 25o of flexion at ball release[5]. At ball release elbow extension velocity peaks at approximately 2500o/sec. The wrist moves into flexion from an extended position and ends in neutral, while the forearm is in about 90o pronation at release.
Muscle activation
Acceleration phase is the most explosive phase of the pitching, and trunk achieves its greatest rotation speed which leads to peak activity of obliques[5].
Strong activity of serratus anterior and pectoralis major continues into acceleration as the shoulder moves into horizontal forward flexion and scapula protracts[8].
Latissimus dorsi becomes active during the late cocking phase as the arm reaches maximum external rotation and continues to contribute towards humeral internal rotation during acceleration phase[9][14].
Subscapularis at its greatest activity as it vigorously moves the arm into internal rotation during this phase. A study was done by Gowan et al[14] found that during the acceleration phase, the contraction of subscapularis, serratus anterior and latissimus dorsi was considerably high in professional athletes compared to amateur athletes.
Triceps is also at its greatest activity during this phase as the elbow violently moves into extension and across the body.
Arm Deceleration Phase
The arm deceleration phase begins at ball release and ends at maximum shoulder internal rotation [3]. Typically the concern in this phase is safely decelerating the forward progression of the arm. Escamilla et al state that a shoulder compressive force slightly greater than bodyweight is generated to resist shoulder distraction, while a posterior shear force of 40-50% of body weight is generated to resist shoulder anterior subluxation. Due to the high forces generated in this phase, the posterior muscles are highly susceptible to tensile overload, undersurface cuff tears, labrum and bicep pathologies, capsule injuries, and internal impingement [3].
It occurs from the point of ball release to maximal humeral internal rotation and elbow extension.
The shoulder is abducted 100o, humeral rotation reaches 0o and arm is horizontally adducted to 35o.
The greatest amount of joint loading is generated during this phase. The posterior shear force of about 400 N, the inferior shear force of 300 N, 1090 N of compressive forces and about 97 N-m of horizontal abduction torque are generated during this phase after ball release.
Muscle activation
This is the most active phase for the muscles of the shoulder girdle as they work eccentrically to decelerate the arm.
Trapezius, serratus anterior and rhomboids produce high MVIC[1] to assist in deceleration of shoulder girdle.
Teres minor presents with its peak activity during this phase as it resists anterior humeral head translation, horizontal adduction and internal rotation.
In addition to teres minor, infraspinatus, supraspinatus and deltoid also present high MVIC to decelerate the arm in space as it moves forward.
Biceps brachii and brachialis produces marked eccentric contraction to decelerate the elbow extension and forearm pronation[2].
700+ accredited online courses for clinicians
Join the world's largest community of rehabilitation professionals
Follow-through
Follow-through is the phase where the body continues to move forward until the arm has ceased motion.
The elbow undergoes a rebound effect and is approximately flexed to 45o[2].
During this phase, the rest of the body catches up with the arm and it culminates with the pitcher in a fielding position.
Muscle activation
During the follow-up phase, the trunk extensors work concentrically to bring the trunk in an upright position. And as the rest of the body catches up with the arm, the pivot leg hip flexors move the leg forward and the pitcher assumes a fielding position.
Common Injuries
Shoulder injuries
Injuries to the shoulder are most common baseball pitching and more particularly in the late cocking and deceleration phase[15]. Following is the list of potential shoulder injuries in different phases of pitching[1].
Windup - No injuries are common.
Cocking - Anterior subluxation, internal impingement, glenoid labrum lesions, subacromial impingement.
Acceleration - Shoulder instability, labral tears, overuse tendinitis, tendon ruptures.
Deceleration - Labral tears at the attachment of long head of biceps, subluxation of the long head of biceps by tearing off a transverse ligament, lesions of the rotator cuff.
Follow Through - Tear of the superior aspect of glenoid labrum at the origin of the biceps tendon, subacromial impingement.
Elbow injuries
Elbow injuries are the second most common injuries in baseball pitching.
Excessive valgus strain at the elbow during the late cocking phase can lead to medial elbow injuries such as muscle tear, avulsion fractures, ulnar nerve damage and most commonly UCL strain or tear [15]. In addition to the valgus strain injuries also follow due to lateral compartment at the elbow such as avascular necrosis, osteochondritis dissecans, osteochondral chip fractures or any combination of this injury [1].
During the acceleration phase, secondary to the excessive elbow extension peak velocity, olecranon can impinge against the medial aspect of the trochlear groove and fossa which may form posteromedial osteophyte and loose bodies formation leading to valgus extension overload syndrome.
References
- ↑ Jump up to:1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Houglum PA, Bertotti DB. Brunnstrom's clinical kinesiology. FA Davis; 2012.
- ↑ Jump up to:2.0 2.1 2.2 2.3 2.4 Seroyer ST, Nho SJ, Bach BR, Bush-Joseph CA, Nicholson GP, Romeo AA. The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention. Sports Health: A Multidisciplinary Approach. 2010 Mar 1;2(2):135-46.
- ↑ Jump up to:3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 Escamilla R, Andrews JR. Shoulder Muscle Recruitment Patterns and Biomechanics during Upper Extremity Sports. Sports Med 2009; 39 (7): 569-590.
- ↑ Zack Greinke Pitching Mechanics Slow Motion Baseball Instruction Analysis LA Dodgers MLB 1000 FPS. Available from: https://www.youtube.com/watch?v=iRPtVfEz4es
- ↑ Jump up to:5.0 5.1 5.2 5.3 5.4 5.5 Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseball pitching A preliminary report. The American journal of sports medicine. 1985 Jul 1;13(4):216-22.
- ↑ Toyoshima S, Hoshikawa T, Miyashita M, Oguri T. Contribution of the body parts to throwing performance. InBiomechanics IV 1974 (pp. 169-174). Palgrave, London.
- ↑ Meister K. Injuries to the shoulder in the throwing athlete part two: evaluation/treatment. The American journal of sports medicine. 2000 Jul 1;28(4):587-601.
- ↑ Jump up to:8.0 8.1 8.2 Moynes DR, Perry J, Antonelli DJ, Jobe FW. Electromyography and motion analysis of the upper extremity in sports. Physical therapy. 1986 Dec 1;66(12):1905-11.
- ↑ Jump up to:9.0 9.1 9.2 9.3 9.4 Park SS, Loebenberg ML, Rokito AS, Zuckerman JD. The shoulder in baseball pitching: biomechanics and related injuries--Part 1. Bulletin of the NYU Hospital for Joint Diseases. 2002 Dec 22;61(1-2):68-79.
- ↑ Jump up to:10.0 10.1 10.2 10.3 Fleisig GS, Escamilla RF. Biomechanics of the elbow in the throwing athlete. Operative Techniques in Sports Medicine. 1996 Apr 1;4(2):62-8.
- ↑ Jump up to:11.0 11.1 11.2 Whiteley R. – ABaseball Throwing Mechanics as They Relate to Pathology and Performance-Review. J Sports Sci Med 2007 6:1-20.
- ↑ Wilk et al. Shoulder Injuries in the Overhead Athlete. J Orthop Sports Phys Ther. 2009;39(2):38-54. Article
- ↑ Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. Journal of Orthopaedic & Sports Physical Therapy. 1993 Aug;18(2):402-8.
- ↑ Jump up to:14.0 14.1 14.2 Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparative electromyographic analysis of the shoulder during pitching professionally versus amateur pitchers. The American Journal of Sports Medicine. 1987 Dec 1;15(6):586-90.
- ↑ Jump up to:15.0 15.1 15.2 Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. The American journal of sports medicine. 1995 Mar 1;23(2):233-9.
- ↑ SPARK Physiotherapy, LLC. The Biomechanics of Throwing. Available from: http://www.youtube.com/watch?v=ERyWx46e7BQ [last accessed 15/06/16]
- ↑ Scotty Gilbertson. Sport Science: Aroldis Chapman. Available from: http://www.youtube.com/watch?v=yEpdoAZiHWQ [last accessed 15/06/15]